CMS-L564 Form PDF Download, CMS-L564 Request For Employment Information PDF, CMS-L564 Form PDF, How To Download CMS-L564 Form PDF, Request for CMS-L564 Form, cms-l564 form download, cms l564 fillable form, can i submit form cms-l564 online, cms-l564 form for spouse, CMS-L564 Form PDF, CMS-L564 Form 2023 Download, CMS-L564 Form 2023 PDF, CMS-L564 Form
CMS-L564 Form PDF Download 2023 : If you have Medicare Part A (Hospital Insurance) and you’re eligible to enroll in Medicare Part B (Medical Insurance) through a Special Enrollment Period (SEP), you have options for how to apply. You can complete the Part B SEP online or you can mail your completed CMS 40B, Application for Enrollment in Medicare – Part B (Medical Insurance) and CMS L564 – Request for Employment Information to your local Social Security office.
You’ll also need to send any required proof of employment, Group Health Plan (GHP), or Large Group Health Plan (LGHP) coverage. You can also fax your enrollment forms and evidence of employment and health coverage to your local Social Security office. You can find your local Social Security office by clicking “SSA Office Locator” under the “Related Links” section below.
Your employer doesn’t need to sign Section B of the CMS L564 form. State “I want Part B coverage to begin (MM/YY)” in the remarks section of the CMS 40B form or the online application. Visit faq.ssa.gov or call Social Security toll-free at 1-800-772-1213 (TTY 1-800-325-0778) for more information. NOTE: If you don’t already have Part A you can apply online at SSA.gov/benefits/medicare.
CMS-L564 Form Purpose – CMS-L564 Form PDF Download
In order to apply for Medicare in a Special Enrollment Period, you must have or had group health plan coverage within the last 8 months through your or your spouse’s current employment. People with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment.
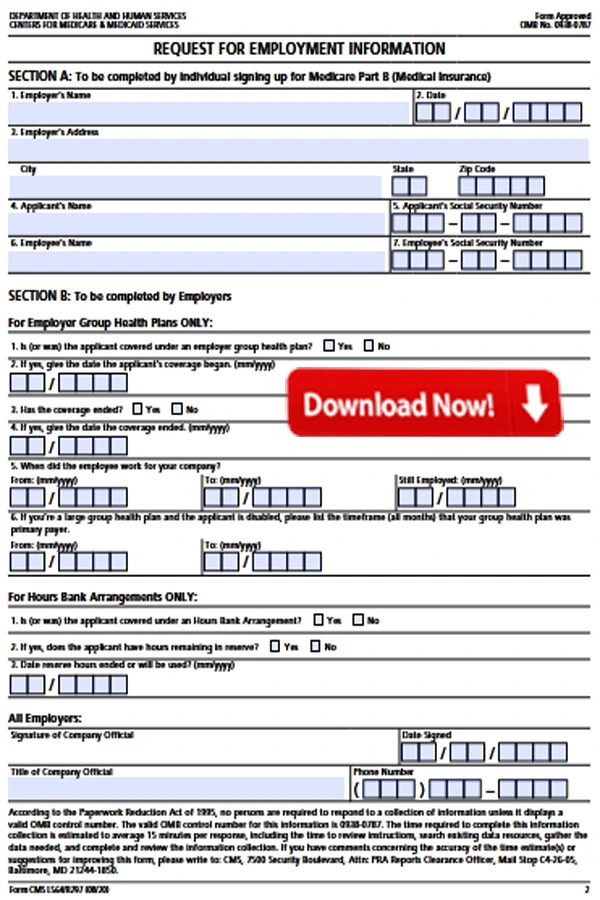
This form is used for proof of group health care coverage based on current employment. This information is needed to process your Medicare enrollment application. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment.
How is CMS-L564 Form filled?
- Complete the first section of the form so that theemployer can find and complete the information aboutyour coverage and the employment of the personthrough which you have that health coverage.
- The employer fills in the information in the secondsection and signs at the bottom.
IRS W-4V Form 2023 PDF Download
How To Fill Form SSA 3820 BK PDF Download
What do I do with the CMS-L564 Form?
Fill out Section A and take the form to your employer. Ask your employer to fill out Section B. You need to get the completed form from your employer and include it with your Application for Enrollment in Medicare (CMS-40B). Then you send both together to your local Social Security office. Find your local office here: www.ssa.gov.
How To Download CMS-L564 Form PDF
CMS-L564 Request For Employment Information PDF — Download PDF
CMS-L564 Form Eligibility – CMS-L564 Form PDF Download
Before diving into the details of how to download the CMS-L564 Form, it’s crucial to understand who is eligible to use this form. This section will outline the eligibility criteria for Medicare beneficiaries, explaining who can request assistance with their premiums and how the CMS-L564 Form plays a vital role in this process.
SSA 827 Form PDF Download
CMS-40B Form Download 2023
Step by Step Instructions for CMS-L564 Form PDF
The person applying for Medicare completes all of Section A.
-
Employer’s name:
Write the name of your employer. -
Date:
Write the date that you’re filling out the Request for Employment Information form. -
Employer’s address:
Write your employer’s address. -
Applicant’s Name:
Write your name here. -
Applicant’s Social Security Number:
Write your Social Security Number here. -
Employee’s Name:
If you get group health plan coverage based on your employment, write your name here. If you get group health plan coverage through another person, like a spouse or family member, write their name. -
Employee’s Social Security Number:
If you get group health plan coverage based on your employment, write your Social Security Number here. If you get group health plan coverage through another person, like a spouse or family member, write their Social Security Number.
Once you complete Section A:
Once Section A is completed, give this form to your employer to complete Section B. Once Section B has been completed by your employer, return this form along with your Part B application to your local Social Security office.
The employer completes all of Section B.
If you’re an employer without an hours bank arrangement, complete the section called “For Employer Group Health Plans ONLY”
s (or was) the applicant covered under an employer group health plan?
Please check yes or no if the applicant was covered under your group health plan offered by your company. The applicant may be the employee or another person related to the employee, such as a spouse or family member with disabilities. If your company doesn’t offer a group health plan, please check No. A group health plan is any plan of one or more employers to provide health benefits or medical care (directly or otherwise) to current or former employees, the employer, or their families.
When did the employee work for your company?
Write the start and end dates of the employment for the employee in which the applicant is related. It may be the applicant or another person related to the employee, such as a spouse or family member with disabilities.
- Enter the month and year of the start of the employment in the “From” box.
- Enter the month and year of end of the employment in the “To” box.
- If the employee is still employed, enter the month and year of the current date.
- Current employment is active working status. It is not disability or retirement.
EPA Form 4700-4 PDF Download And Instructions PDF
SF-424B Form PDF Download
Step-by-Step Guide to Downloading the CMS-L564 Form as a PDF
Now that we have a clear understanding of the form’s purpose and eligibility requirements, let’s walk through the process of downloading the CMS-L564 Form as a PDF. This step-by-step guide will include detailed instructions, screenshots, and tips to ensure a seamless experience for individuals seeking to obtain the form online. The following steps will be covered:
- Accessing the official Medicare website
- Navigating to the forms section
- Locating the CMS-L564 Form
- Downloading the PDF version
Section 4: Completing the CMS-L564 Form (800 words) Once you have successfully downloaded the CMS-L564 Form, the next crucial step is filling it out accurately. This section will provide detailed guidance on how to complete each section of the form, including:
- Personal information
- Employment or group health plan details
- Authorization and certification
Submitting the CMS-L564 Form – CMS-L564 Form PDF 2023
After completing the form, you need to know where and how to submit it to ensure your request for assistance is processed efficiently. This section will cover the following aspects:
- Submission options (mail, fax, in-person)
- Required supporting documents
- Contact information for inquiries
Common Questions and Troubleshooting – CMS-L564 Form 2023
This section will address some frequently asked questions about the CMS-L564 Form and provide troubleshooting tips for common issues that individuals may encounter during the downloading, completion, or submission process.
Form SF 424 PDF Download
IRS Form 5500 PDF Download
Conclusion – CMS-L564 Request For Employment Information
In conclusion, the CMS-L564 Form is an essential document for Medicare beneficiaries seeking assistance with their premiums or other Medicare-related benefits. This comprehensive guide has provided valuable insights into the purpose, eligibility criteria, and step-by-step instructions on how to download, complete, and submit the CMS-L564 Form as a PDF. By following these guidelines, individuals can ensure that they meet the necessary requirements and provide accurate information to access the assistance they need for their Medicare coverage.